


Did digital contact tracing work?
Did digital contact tracing work?
Yes, if done right. Which unfortunately wasn't the case in most places, reflecting the digital underdevelopment of public health systems.

This is part 3 of a 4+1 series on digital contact tracing. You can read the previous parts here:
Part 0: Digital Contact Tracing - a mini series in 4(+1) parts
Part 1: Why contact tracing needs to go digital
Part 2: Privacy in digital contact tracing
___
I’m not going to mince words: In many places, public health is 20 years behind in terms of digital development. There are probably a number of reasons for that - public health is ultimately a mix of medicine and government, both not exactly systemic trailblazers of digitization (note the word systemic - of course, there are individual parts in these systems that are absolutely cutting-edge). Add to this mix a relatively high level of risk aversion, and it’s no wonder that some otherwise highly advanced countries still used fax to send around case reports of COVID-19. But that is a story for another time.
So, did digital contact tracing work? We’d ultimately like to have a systematic review of the data, but it’s too early for that. The EU recently published a relatively thorough report on digital contact tracing. It has some interesting numbers in it:
Data analysis across the investigated countries revealed that, since their launch in 2020 and until July 2022 the apps reached the number of 206 million unique voluntary downloads. The number of active users reached up to 45% of the total population. In six of the studied countries where the apps have been most intensely used (Finland, Ireland, Germany, Iceland, France, Switzerland), the percentage of active users per total population ranged between 26 and 45% and the numbers of peak active users added up to 56 million active users. Up to 70% of app users who were diagnosed positive with COVID- 19 entered their test results in the app to warn others. Across the studied apps, over 13.4 million positive tests were entered into the apps to warn other people at risk of infection, with best practices showing that the number of positive tests entered into the app can reach up to 20% of the total number of positive cases in the respective country. Countries reported that between 0.8 and up to 19 exposure notifications per positive entered test into the app were sent to notify contacts at possible risk of infection. Data reported from seven countries revealed that over 177 million warning notifications have been generated.
Digital contact tracing was part of health systems’ resilience response to a new situation, developed at a very fast pace related to other innovations, and adopted at a considerable scale in a voluntary manner by a higher than expected amount of the population. This effect is particularly striking, in the sense that not everyone immediately accepts a disruptive idea. In the context of contact tracing apps, an unprecedented large adoption of a new digital public health technology was observed in several countries.
Here, I’m going to report on the first three studies that I am aware of looking at empirical evidence.
As digital contact tracing solutions were being deployed on a large scale, the question of effectiveness naturally emerged. Not having been tested in the field before, digital contact tracing was a technology without evidence that it worked, even though the model predictions were clear that it should. In addition, there was no a priori reason to assume that the digital version of contact tracing should be any less effective than the manual version. In fact, the hope was very much that digital contact tracing would be much more effective than conventional contact tracing, even if just because of speed.
The decentralized nature of digital contact tracing meant that there was no centralized data that could retrospectively be analyzed. Recall that the central system does not know anything about contacts, or who had received an exposure notification. This was a desired property of the system from a privacy perspective, as discussed in a previous post - but it meant that the necessary data for an assessment of efficacy would have to be gathered in another way. In what follows, we will look at three different approaches to GAEN-based apps from Switzerland, Spain, and the UK.
Switzerland
The Swiss study - to the best of my knowledge the first with real-world data - looked at the time period shortly after the launch of the country’s digital contact tracing app “SwissCovid”, from July to September, 2020. COVID-19 cases were relatively low at the time, as the large fall wave hadn’t started yet. In the study time period, 1,645 activation codes were entered into the app, and 16.7% of the Swiss population actively used the app. It is not precisely known how many notifications were triggered by the app, but the system led to 1,695 phone calls to the SwissCovid hotline (calling that hotline was a recommended step by the app after receiving a notification). Most RT-PCR test protocols included a question about whether the subject getting tested had received an exposure notification. During the study period, this number was estimated to be 65 (95% CI 54–77). Thus, the number of positive contacts per index case could be estimated as ε = n/(cμ), where n = 65, c = 1,645 and μ = 16.7%. This formula assumes that contacts of app users are themselves app users with a probability μ, and thus ε = 0.24 (95% CI 0.20 - 0.27), a range similar to numbers reported in conventional contact tracing studies at the time.
Spain
An entirely different approach was taken in Spain, which had developed the “RadarCovid” app. To assess effectiveness, a simulation experiment was designed, taking place on an island (La Gomera, one of Spain's Canary Islands). The local population was invited to participate in an experiment where simulated infections would trigger exposure notifications. Between 29th June and 22nd July 2020, an estimated 33% of the local population of ~10,000 downloaded the app, and four outbreaks were simulated in that time period, where roughly 10% of app users were simulated as infected. Through extensive follow-ups and online surveys, numerous key performance indicators were assessed, including compliance, turnaround time, follow-up, and hidden detection, referring to the percentage of contacts that were strangers to the index case. Overall, the study showed high compliance (64% of users getting an activation code entered it into the app), and detected an average of 6.3 close contacts per simulated infection, about twice the yield from conventional contact tracing. Between 23% and 39% of exposed contacts were strangers to the index case, highlighting a key strength of digital contact tracing. The average time between inserting the activation code in the app, and the recommended follow-up call of the contact was 2.35 days, which was slightly faster than the comparable time period reported for conventional contact tracing of 2.6 days. However, only about 10% of the notified contacts followed up by making this call. Whether this low rate was related to the fact that participants were aware of the simulated nature of infections could not be evaluated. Overall, the study suggested that digital contact tracing worked correctly, and provided experimental, even if simulated, evidence for its usefulness, while at the same time highlighting the critical aspect of population support for the method.
England and Wales
The strongest empirical evidence to date for digital contact tracing comes from England and Wales. The National Health Service NHS had initially advanced in developing a centralized contact tracing app, but switched to the GAEN protocol in the summer of 2020, and launched the “NHS COVID-19” app on September 24, 2020. Upon installation of the app, users were prompted to enter their postcode district, which allowed for geographical analyses (see Figure below). Between app launch and the end of the year, i.e. during the fall wave of 2020, the app was used by approximately 28% of the population. The app triggered approximately 1.7 million exposure notifications - an estimate based on data reported anonymously to the health authorities by the app - which corresponds to 4.2 notified contacts per index case. In comparison, conventional contact tracing triggered 1.8 contact notifications per index case, and thus like in Spain, the yield of digital contact tracing was substantially higher. The secondary attack rate (SAR) was estimated at 6%, which was similar to the SAR for manually traced contacts.
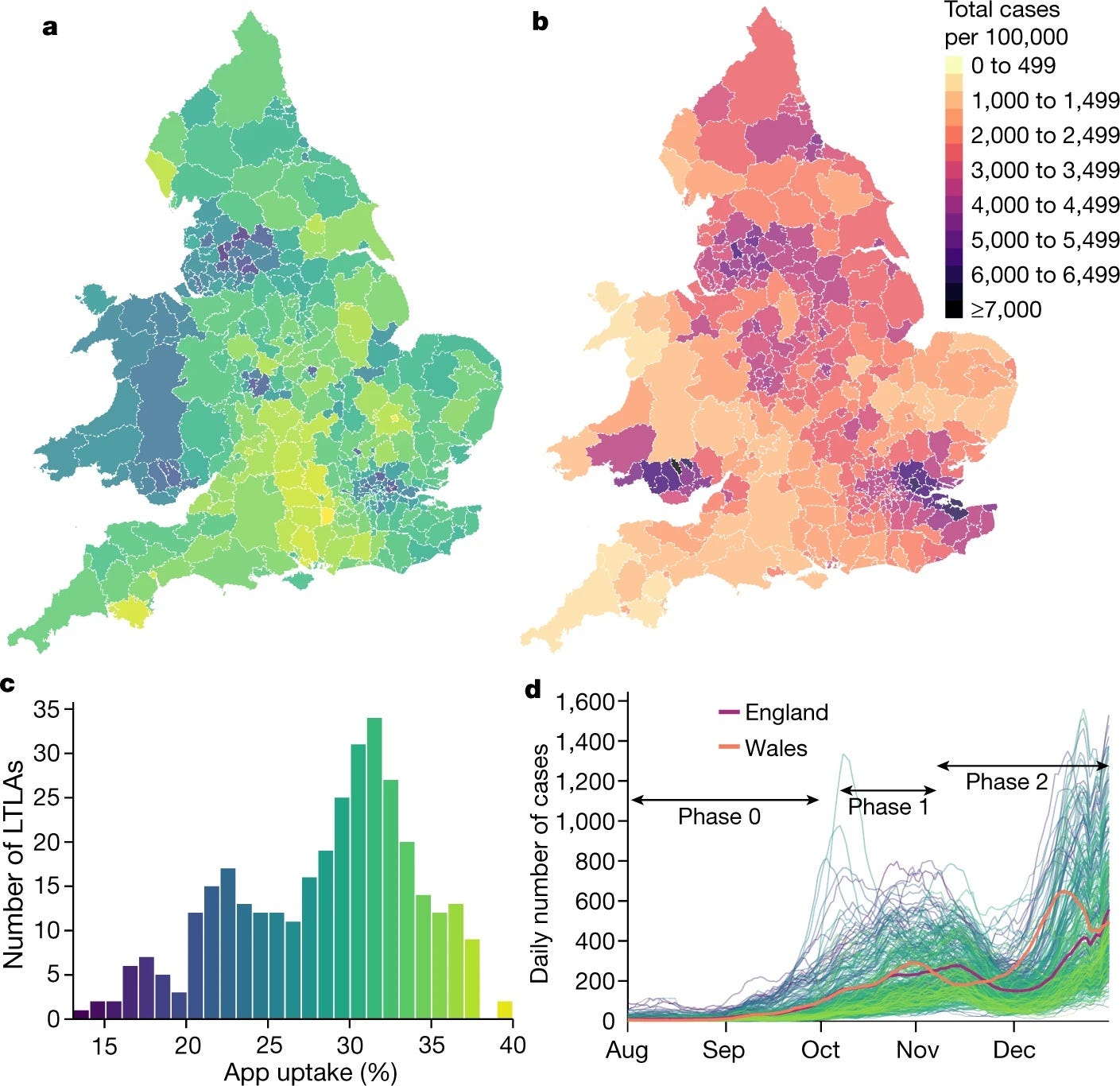
To understand the epidemiological impact of the app, the study used two complementary approaches. The first was to use a modeling approach to understand the effect of a notification, which took into account the number of notifications, the SAR, the expected fraction of transmissions prevented by quarantine, quarantine adherence, and an estimate of the expected size of the transmission chain that would occur in the absence of the notification. The second approach leveraged the fact that app users indicated their postcode district upon app installation. An analysis at the level of local authorities linked geographic variation in app uptake with geographic variation in cumulative case counts, taking into account confounding factors at the geographic level. Both analyses estimated that during the study period of a bit more than 3 months of the fall 2020 wave, digital contact tracing prevented between 284,000 and 594,000 cases, with the combined 95% sensitivity analyses showing a range of 108,000 to 914,000 cases prevented. Correspondingly, taking fatality rates at the time into account, the estimates for averted deaths due to digital contact tracing were 4,200 to 8,700 (1,600 – 13,500). Further analysis showed that for every percentage point increase in app uptake, the number of cases averted was 0.8% (using the modeling approach) and 2.3% (using the geographical analysis):

Overall, such studies provide emerging evidence that digital contact tracing is an effective addition to the arsenal of tools to fight infectious disease outbreaks. The EU report mentioned above concluded that “best practice examples show that the apps can be a powerful tool to complement conventional contact tracing and support public health processes, by consistently identifying contacts that tested positive which would otherwise be missed by conventional contact tracing”. While more analyses will likely be forthcoming, the current evidence suggests that decentralized digital contact tracing can fulfill its key promises of providing rapid notifications to relevant contacts, including many that would not be notifiable through conventional contact tracing, all while strongly preserving privacy. In doing so, it can prevent cases and deaths, but its efficacy very much depends on app uptake rates and proper integration into the test-trace-isolate-quarantine pipeline. Initial fears about rampant false-positive notifications overwhelming the healthcare system did not materialize.
In the next, and final post of this series, I will discuss key learnings from our experiences with digital contact tracing.